If it were stylistically appropriate for me, I’d be hollering “Haleluiah!” and jumping around:


If it were stylistically appropriate for me, I’d be hollering “Haleluiah!” and jumping around:
Glial cells are part of the nervous system, kind of woven throughout it, appearing more densely in some areas (the brain) than others (the fingertips.) They were formerly considered to be just support structures, but I remember, back around 1990, reading articles linking them to inflammatory processes in the brain. Therefore I figured they were part of the brain’s immune system, but science (and funding) didn’t make that short leap (inflammation to immune response) until recently. Now they’re considered key to the brain’s own immune system.
Astrocytes (‘astro’ means star; ‘cyte’ means cell) are a type of glial cell, named for their spiky, roundish, star-like shape. This article says that, in fruit flies at least, astrocytes regulate the sleep/wake cycle:
This is interesting because the circadian rhythm is disrupted in CRPS, and we’ve recently learned that astrocytes and other glial cells are disrupted by CRPS too. Assuming human’s astrocytes are functionally similar to fruit flies’ astrocytes, that circadian rhythm issue might be caused — or at least mediated — by those twinkling astrocytes.
I have several topics competing for attention:
– The lowdown on neurotransmitters: what they are, what they do, where and how they’re made.
I can’t find my old version, but I’d rather rewrite it anyway and lard it heavily with current references and links.
– After that, there’s more to say about how neurotransmitters can be affected — for better or worse — by what you do, what you eat, and how you use your noggin.
This is aimed at that helpless feeling we tend to get when our minds go awry. There’s a lot you can do to mend your mind from the inside out, either with med help or without. I’d like to put the main strategies together here, because so much advice seems conflicting. Mostly, it isn’t, but it would be good to see why.
– Putting the “might” back in mitochondria: how to support your mitochondria in sickness and protect them in health.
This goes into the mechanics and physiology of the reparative stuff I mentioned in the prior article on mitochondria.
These are the big 3. Any preferences?
This replaces “The Dominance of Duh,” a diatribe written in a haze of detox from overmedication. This post should be more useful.
“First, do no further harm.”
It’s the most important treatment guideline there is.
Why is that so relevant? Because Nature doesn’t give the body a free pass, just because the poison comes with a prescription. Physics and chemistry are not impressed by education; they do exactly what they are supposed to do, regardless of who’s watching them… Or failing to.
Therefore, prescriptions don’t alter the nature of what’s being prescribed. Every assault on the body — however therapeutic it’s intended to be — triggers a response involving the nerves, inflammation, and immune system. Medications affect the liver and kidneys, and probably the intestinal system as well.
That’s a lot to affect.
How do you deal with this in the real world, as a real person with real conditions requiring real medication?
Well, good friends help. So does communication. Here’s why:
Your doctor/practitioner is supposed to do a risk-benefit analysis of each drug prescribed. Some take this more seriously than others, some weigh the risks differently, and each practitioner has a unique idea of what’s really important in the first place. It’s good to be aware of your practitioner’s priorities and beliefs, so that their decisions make more sense to you, and you can be better aware of what to ask about or follow up on.
Communication: Get the lowdown on the treatment from your doctor, your pharmacist, your nurse friends. It can be confusing at first since everyone has their own ideas, but the common themes (and common concerns) will emerge, giving you something to look into more closely. Also, they can tell you what terms to use when you go to look it up online.
Good friends: One reason we have friends is so we don’t have to hold everything in our own heads: we can talk things over with them, and then go back for reminders. Another is because they can help us clarify our thinking, and if your meds can make you a bit confused, that’s essential! It’s important to have friends who can tell you when you’re a mess, and maybe it’s time to get your meds re-evaluated.
Need to get your meds re-evaluated? That brings us back to communication, and talking things over with your doctor. It’s a perfectly reasonable thing to ask, so feel free to: medically speaking, it’s good practice to do this periodically. Bring a friend to the appointment, if that would help you discuss it.
Three more things you can do, essential to health: drink plenty of water, eat plenty of produce, and get a bit of fresh air every day. These help your body clear out the excess, keep your natural detox systems working, and provide your body with the building blocks for recovering from the chemicals — either the added chemicals of medication, or the stress chemicals your body releases around treatments and procedures, or both.
Being a patient is a tough job. We have to trust our beings to people who aren’t us, and that entails a certain amount of risk. It’s EXTREMELY easy to blame doctors for screwing up, but when all is said and done, we own our share of responsibility in that relationship.
So talk to your doctor. Talk to your friends. Drink up and eat your greens. Now let’s take a nice walk …
Without mitochondria, you have no way of converting food into energy.

When you were being conceived, half your cells’ genes came from your mother and half from your father. All of the other stuff that goes inside a cell came from your mother. This includes the mitochondria. (This is why mitochondrial DNA is used to track maternal inheritance: it always comes down the female line.) Your mother’s cell hosts conception, just as (normally) your mother’s body hosts gestation.
Mitochondria have a fairly smooth outer layer and a deeply-rumpled inner layer. Most of the action happens inside the rumpled layer. This is where the ribosomes, most of the fluids and loose protein, and the ATP-making particles hang out.

Cells, including mitochondria, need various proteins to do their work with. Large proteins get carefully handed from the outside world, through the outer layer of the mitochondrion (singular of “mitochondria” — sorry, it’s still Greek), then into the inner layer.
If the smooth outer layer is damaged, this makes this transfer process screw up, and the inner layer gets disrupted, ripping up the cell. Granules and nucleic acids all over the place. Bang goes that ATP production.

Those are some busted mitochondria.
This kind of damage happens in response to certain kinds of toxins (including certain medications for AIDS and all psychoactives — including antidepressants and pain medications, which seems especially mean!), occasionally from genetic disturbance, and occasionally as a consequence of illness — or nerve injury and its complications.
Mitochondrial dysfunction has been repeatedly and profoundly linked to neurogenerative diseases like Alzheimer’s and Parkinson’s; cell-metabolism problems like heart disease, insulin resistance and type II diabetes; and several diseases often mistaken for CRPS.
Not surprisingly, symptoms of mitochondrial dysfunction are the worst in tissues that use the most energy and have the largest number of mitochondria per cell: nerves, muscles, brain.
Recently, it has been strongly associated with CRPS. And the cherry on top: it plays a vital role in neuroplasticity, or the way your nerves and brain change — for better or worse.
Hell-o, “pain-brain.” We thought we knew ya!
Knowing why it’s so damnably exhausting to walk a mile, when it used to be fun — fun! — to run 3, is a bit of a relief. First question that leaps to my mind: How do I fix ’em? How do I give them what they need to get better and protect themselves? The answer seems simple: antioxidants are what’s needed to prevent and repair that damage (good explanation of that here) to the walls of the mitochondrial cell. Mitochondria are both the biggest makers of reactive oxygen species and the biggest scavengers of them, so of course it makes sense that that’s exactly the kind of help they need when they can’t keep up.
Downing antioxidants by the bucketful is one way to get them in. Intriguing for three reasons:

Kind of depressing for one simple reason: it’s iffy whether, once you’ve got the disease process going, the antioxidants can get where they’re needed and save your poor beleaguered mitochondria. … Having said that, I notice that the writers of that article seem to be trying to sell something, and that makes me very suspicious of their conclusions.
Next, I’ll offer suggestions for patients, suggestions for clinicians, and then wind this up with a foray into the question of whether mitochondrial issues have a genetic component, like being X-linked — the way a cat’s fur color is!
Two things that you hardly need reminding of:
Most antioxidants are not going to hurt you, without letting you know first (that is, make you nauseous or feel funny.) Take vitamin C in doses no larger than 500mg, since larger doses tend to trigger your gut to throw the C away. Go ahead and try stress-vitamins, co-enzyme Q-10, N-acetylcysteine, hair-skin-&-nails vitamins (these are really fat-soluble antioxidants) … try things, take what helps, and put aside the rest if they don’t do anything. Keep in mind that things change: what doesn’t work now might work later, and vice-versa.
For antioxidant powerhouses, look for dark-red and dark-blue fruits: pomegranates, blueberries, red wine, chocolate (though some CRPS people have to avoid that for its nerve effects), mangosteen (my favorite fruit), cranberries, and so on.
Most treatment standards, particularly for CRPS, are based on science that’s over a decade old. They shouldn’t be changed blithely but they can certainly be improved. There is plenty of room for that.
The following points are intended as additions to the standards you follow for CRPS, as they are good guidelines for mitochondrial and neurologic support in a system compromised by CRPS.
These ranges are empirical; if you can find the funding to do the science to develop more reliable ranges for this population, so much the better.
Adequate tissue oxygenation and perfusion can return substantial function and significantly reduce pharmacologic burden. Patients can demonstrate this, even where the data have not been published and peer reviewed. Therefore, use antioxidants rigorously and intelligently.
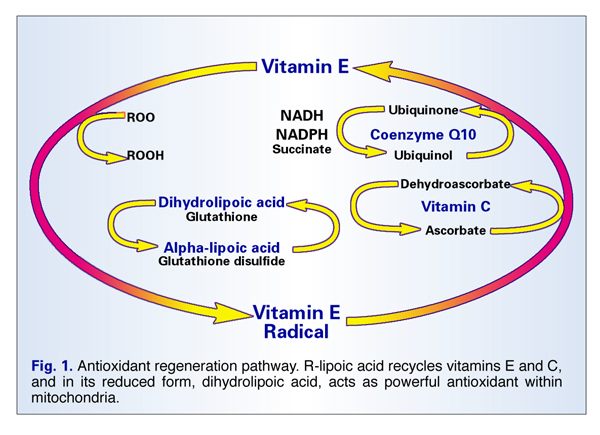
Image credit: http://www.vrp.com/antioxidants/-r-lipoic-acid-unique-mitochondrial-antioxidant-fights-premature-aging. (Article’s not bad.)
Why all that anti-oxidation when the medical literature is not definitive? 2 reasons, which you ought to know for yourselves:
Keep in mind that doctors are not the only scientists interested in the human body. Be prepared to look into other disciplines for leads when your own offers no good options.
Try Nursing, PT, Nutrition, Therapeutic Massage — you’ll realize that nobody knows more about soft tissue’s functional physiology in vivo than therapeutic massage science, and if nothing else, the exercise in intellectual flexibility might do you good.
The accepted style is very different, but the info they have is tremendous.

Forward-looking thoughts:
Let’s go back to mitochondria in reproduction. Kind of in an X-rated way, figuratively speaking.
We know that women have two X chromosomes. The Y chromosome is a stubby little object with hardly any data to use, unless you’re into color-blindness or hemophilia; this means women have quantities of extra data, which can have even more devastating effects (as in, Down syndrome.) So how to handle the extra genes?
Pick one. Simple as that.
Shortly after conception, when the cells are just dividing like mad and haven’t decided what to be yet, every single cell turns off one of its two X chromosomes; each of that cell’s daughter cells inactivates the same X chromosome. As the cells continue to multiply, then fill out, fold, bend around, and specialize, to become a whole, separate being, it means that X-linked traits appear in a mottled pattern throughout the body, as the two sets of daughter cells continue reproducing and passing on their particular X-activations. Isn’t that curious?
As an especially decorative instance, cats’ hair color is an X-linked trait:
Cool, huh? Love her accent, too.
But this fact brings me to a serious question about mitochondrial disease. If mitochondria are sex-linked, is there a relationship between the X chromosome and mitochondrial expression? It seems improbable that there wouldn’t be, because mitochondria reside inside the cell, and the cell’s action is determined by the genes within it. The mitochondria had to have developed a special relationship with the X’s in the 23rd chromosomal pair, after all those millenia.
It’s generally accepted that mitochondrial diseases are due to toxification or to complex, multigenetic issues. Ok, fine. But what about mitochondrial vulnerabilities that don’t become pathologic until they are damaged in some other way? To what degree is toxification an issue related to X-activation? In other words, is mitochnodrial vulnerability related to vulnerabilities in the active X chromosome?
Is there a patchy characteristic to the early stages of mitochondrial destruction? — You know, the early stages of rare disorders, the time when it’s impossible to get a diagnosis because the doctors are all so busy chasing their own tails around your irrational symptoms and their own ignorance.
Is that initial “mottled” activity one reason why these diseases are so damn weird?
Link list:
Wikipedia’s entry on mitochondria is pretty good:
http://en.wikipedia.org/wiki/Mitochondria
On mitochondria and AIDS meds:
http://www.ncbi.nlm.nih.gov/pubmed/20818734
On mitochondria and pyschoactives:
http://www.ncbi.nlm.nih.gov/pubmed/18626887
Alzheimer’s Foundation:
http://www.alzfdn.org
Michael J. Fox’s Parkinson’s foundation:
http://www.michaeljfox.org/
United Mitochondrial Disease Foundation, listing diseases which are often mistaken for CRPS:
http://www.umdf.org/
Mitochondria and neuroplasticity:
http://www.ncbi.nlm.nih.gov/pubmed/20957078
A good rundown (so to speak) of antioxidants’ function:
http://www.ionizedwateronline.com/Antioxidants.html
Vitamin C around surgery.
Upper limb:
http://www.ncbi.nlm.nih.gov/pubmed/17606778
http://www.ncbi.nlm.nih.gov/pubmed/20224742
Lower limb:
http://www.ncbi.nlm.nih.gov/pubmed/19840748
Vitamin K and CRPS progression:
http://www.ncbi.nlm.nih.gov/pubmed/20378261
Getting antioxidants where they’re most needed. Ignore the shystering towards the end:
http://www.ncbi.nlm.nih.gov/pubmed/21422516
ALA and regeneration of Vitamin E:
http://www.vrp.com/antioxidants/-r-lipoic-acid-unique-mitochondrial-antioxidant-fights-premature-aging
